
 After World War II, the U.S. saw a dramatic shift in dietary patterns, encouraged by large food corporations that promoted processed, shelf-stable foods. This era marked the beginning of a strategic demonization of fats—particularly saturated fats—in favor of carbohydrates.
After World War II, the U.S. saw a dramatic shift in dietary patterns, encouraged by large food corporations that promoted processed, shelf-stable foods. This era marked the beginning of a strategic demonization of fats—particularly saturated fats—in favor of carbohydrates.
Recognizing that a low-fat diet would naturally lead people to consume more carbohydrates, sugar executives devised a strategy. They anticipated that dietary habits would pivot towards carbohydrates by about 20 percent, which would greatly benefit all carbohydrate-related industries [1]. To ensure this shift, in 1967, these executives funded Harvard scientists to produce a review that downplayed the harmful effects of sugar and instead implicated fats and cholesterol as the primary culprits of heart disease [1].
This manipulation of science was not isolated to the sugar industry; the vegetable oil and other carbohydrate-centric industries also played significant roles, profiting immensely from the increased consumption of their products as public health declined. Now, half a century later, diabetes and obesity among children and adults have skyrocketed.
Cholesterol is a complex molecule essential for hormone production and cellular structure. It is transported in the body by lipoproteins, which include LDL (low-density lipoprotein) and HDL (high-density lipoprotein). LDL, often misleadingly labeled as “bad” cholesterol, carries cholesterol from the liver to other parts of the body. HDL, commonly known as “good” cholesterol, helps transport cholesterol from the body back to the liver for processing and elimination.


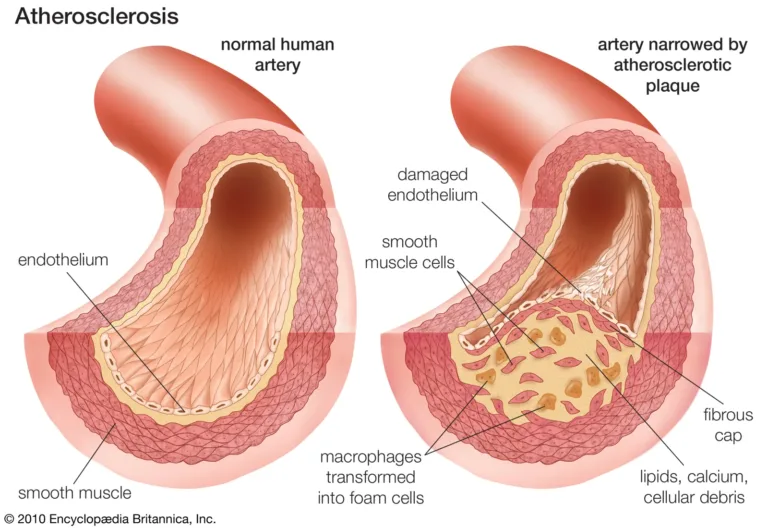
It was once believed that high LDL levels would lead excess cholesterol to build up on the walls of blood vessels and therefore cause the cascade of calcification leading to atherosclerosis. However, this is not entirely accurate.
The actual precursor to heart disease is inflammation that weakens and damages the blood vessel walls [3]. This endothelial damage is often caused by metabolic disorders like diabetes and high blood sugar, chronic infections such as Chlamydia Pneumoniae, smoking cigarettes, heavy metal toxicity, and high blood pressure [4,2]. These factors can cause LDL to accumulate where endothelial damage already exists, worsened by phagocytes that adhere cholesterol to these vulnerable areas [3].
Additionally, research shows that high LDL levels are often a response to underlying metabolic and immune disorders [5]. Cholesterol can accumulate in macrophages and other immune cells, promoting inflammatory responses in an effort to neutralize or contain the threat. This response is initially beneficial; however, when this mechanism becomes chronic or unbalanced, it can contribute to the development of atherosclerosis in a vicious cycle [5].
Instead of addressing these root causes, conventional approaches often focus solely on reducing cholesterol levels. This overlooks the underlying factors such as chronic infections, metabolic disorder, and toxin exposure, and it often creates new problems for patients as well.
Statin drugs are widely prescribed to lower cholesterol as a strategy to reduce the risk of heart disease. They work by inhibiting a key enzyme in the liver responsible for cholesterol production, effectively lowering levels of LDL cholesterol. However, emerging research challenges the robustness of these benefits. Studies indicate that while statins do effectively lower LDL cholesterol, this does not always translate into a significant reduction in cardiovascular events [6]. In fact, they do not prevent heart disease in 98.8% of patients [6]. This discrepancy raises questions about the universal effectiveness of LDL reduction as a preventive strategy and lifestyle medicine.
 Moreover, statins can disrupt the synthesis of Vitamin K2, a crucial nutrient for cardiovascular health. K2 activates the Matrix GLA Protein (MGP) which prevents the calcification of blood vessels, thereby maintaining their flexibility [7]. It also plays a key role in regulating calcium deposition, ensuring calcium is directed to the bones rather than accumulating in the arteries. The inhibition of Vitamin K2 synthesis by statins can lead to increased arterial stiffness and contribute to cardiovascular risk, contrary to their intended use [8].
Moreover, statins can disrupt the synthesis of Vitamin K2, a crucial nutrient for cardiovascular health. K2 activates the Matrix GLA Protein (MGP) which prevents the calcification of blood vessels, thereby maintaining their flexibility [7]. It also plays a key role in regulating calcium deposition, ensuring calcium is directed to the bones rather than accumulating in the arteries. The inhibition of Vitamin K2 synthesis by statins can lead to increased arterial stiffness and contribute to cardiovascular risk, contrary to their intended use [8].
There are also concerns about the broader impacts of artificially lowering cholesterol levels. As we discussed, cholesterol is essential for cell membrane structure and the production of certain hormones. Excessively low cholesterol, driven by statin use, can be associated with cognitive decline including dementia, hormone imbalances, and other health complications [9].
Adding complexity, the shifting laboratory reference ranges for LDL cholesterol, influenced by the widespread use of statins, have altered what is considered “normal.” As more people use statins, the average LDL levels decrease, shifting the lab reference ranges downward. This shift can lead to overdiagnosis of high cholesterol in individuals who, under previous standards, would have had normal LDL levels.
For a deeper understanding of lab reference ranges and interpreting results, you can read more on our blog: Beyond Normal: Understanding Your Lab Results.
 Understanding cardiovascular health extends beyond the simple metrics of LDL cholesterol and dietary fat intake. It’s about supporting the body’s natural processes with the right nutrients and making informed choices about medical treatments. We encourage our patients to adopt a holistic view of their health, focusing on true indicators of cardiovascular well-being and ensuring their bodies are supported with the necessary nutrients for optimal health.
Understanding cardiovascular health extends beyond the simple metrics of LDL cholesterol and dietary fat intake. It’s about supporting the body’s natural processes with the right nutrients and making informed choices about medical treatments. We encourage our patients to adopt a holistic view of their health, focusing on true indicators of cardiovascular well-being and ensuring their bodies are supported with the necessary nutrients for optimal health.
Ready to take control of your heart health? Schedule a consultation with us today!




